In the last week, as the Federal government comes towards next Tuesday's annual fiscal statement…
COVID-19 myopia – it actually costs more to have no acute care protocols in place and more people die as a result
I regularly scan research output from disciplines other than economics that I think impacts on economic matters. On April 17, 2024, a new study from medical researchers at the Burnett Institute in Melbourne, working with staff at the Department of Health and Human Services, in Victoria published a pre-print in The Lancet – Admission Screening Testing of Patients and Staff N95 Masks are Cost-Effective in Reducing COVID-19 Hospital Acquired Infections – which continues to show that public health policy in Australia is failing and part of that failure is the myopia that ‘sound finance’ principles engenders. I have written before about this myopia where governments think they need to cut back on spending because they are ‘short’ of funding and end up having to spend more over time because the initial spending cuts cause massive (and predictable) problems. We have seen this phenomenon in many situations (several cases are cited below). This new research puts an end in my view to the debates about hospital and more general health practices in the Covid era and exposes how the lack of political leadership, a refusal to fund public education, and poor hospital practices – mostly due to alleged funding shortfalls – have turned Australian hospitals into death zones. And while the authorities are telling the public they are ‘saving taxpayers’ money’ the reality is that the pubic outlays to deal with the problems they are creating by this austerity will be multiples of what would be required to implement sound policy now and avoid those longer-term problems.
There are countless examples now of this type of neoliberal myopia and I have covered them in these blog posts (among others) over many years of study:
1. More privatisation myopia (March 22, 2021) – privatisation of world-leading vaccine producer in Australia.
2. Neoliberal myopia strikes again (December 16, 2020) – long-term impacts of cuts in health infrastructure.
3. Mental illness and homelessness – fiscal myopia strikes again (January 5, 2016) – housing and homelessness.
4. British floods demonstrate the myopia of fiscal austerity (January 4, 2016) – British flooding
5. The myopia of fiscal austerity (June 10, 2015) – British canal rat infestation and collapse of Manchester sewers.
6. The myopia of neo-liberalism and the IMF is now evident to all (October 8, 2014) – long-term income losses from austerity.
7. Myopic meanness – Australia’s ODA cuts to its neighbours in the Pacific (April 5, 2022) – loss of strategic geopolitical position due to cuts to foreign aid.
8. Australia’s bushfire dystopia – another entry for the neoliberal report card (January 9, 2020) – refusal to fund climate transition and bushfire damage.
The research paper I cited in the introduction comes from the – Burnett Institute – which is a world-leading medical research group that “combines medical research in the laboratory and the field, with public health action to address major health issues affecting disadvantaged communities in Australia, and internationally.”
It specialises in infectious disease research and helps design public health programs in Australia, Africa, Oceania and Asia.
It provided early and leading research in the study of HIV, influenza and STDs.
In this latest research, we learn that previous claims that N95 mask-wearing makes no different to the spread of Covid especially in hospital settings, which have been weaponised by policy makers intent on ‘saving’ health expenditure, do not stack up.
The research was motivated by the on-going debate about how to deal with life-threatening infections in health care settings.
That is, a person enters a hospital for a routine operation expecting to come out soon enough after surgery, but, instead catches Covid, becomes very ill, and dies in the hospital.
That type of phenomena is rising in incidence although authorities are reluctant to publish the (embarrassing data).
A dear friend of mine lost his long-time partner recently after she was hospitalised after a fall but acquired Covid in the hospital and never came out.
A UK study found that “11.3% of hospitalised COVID-19 patients acquired COVID-19 whilst in hospital …, 11.8% in Germany … and 9.2% in Brazil …”
Between 2020 and 2022, Australian hospital workers were required to observe strict protocols to reduce these types of infections.
However, under pressure from the vocal anti-vax, freedom lobby combined with an obsessive quest for a fiscal surplus (to ‘save’ money) the Australian government relaxed all the pandemic orders in 2023 and left it up to individual entities to implement whatever infection control and prevention protocols they liked.
And the funding was severely cut, which placed pressures on the health care providers (hospitals, clinics etc) to reduce the procedures to, in some cases, nothing!
The results have been obvious – “many acute care settings have ceased testing patients on admission” and abandoned the use of N95 masks all while COVID-19:
… continues to cause epidemic transmission and impacts.
Within this context, the Burnett researchers noted that:
… there is limited understanding of the most cost-effective ways to reduce infections, in particular COVID-19 hospital-acquired infections.
They sought to quantify:
… the cost benefits of different patient testing and mask types in acute care facilities, as well as evaluating and comparing the efficacy of these interventions applied continually versus only during periods of high COVID-19 prevalence.
They deployed an ‘agent-based model’ calibrated with real world health data to simulate different cost trajectories and then analysed these trajectories by “comparing different configurations of patient admission screening testing and staff mask usage”.
I won’t elaborate on their research techniques but they are sound.
They modelled three different types of interactions within acute wards – “patient-patient, staff-staff, and staff patient”.
They didn’t model visitor impacts but suggest that their outcomes are understated because of this.
They modelled different testing protocols – PCR and RATs as well as the use of N95 masks as opposed to the less protective surgical masks.
Data was supplied by the Victorian Health Department.
Taken together they then calculated different health outcome scenarios (excluding Long Covid cases – which means they again understate the severity) and then applied input data to each simulated scenario to assess the total costs of each in 2023 $A terms.
The cost inputs were interesting and represented by this Table.
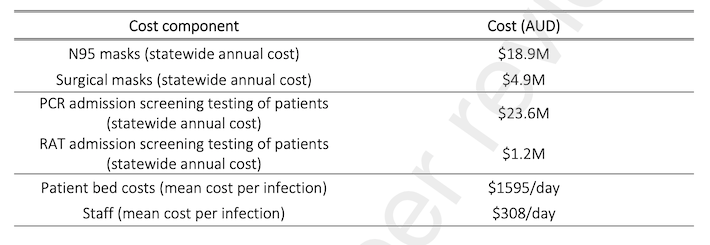
It is obvious that massive savings to government arise from scrapping any mandates to wear N95 masks and to screen for Covid on admission.
You can also see the cost of each infection per day.
What becomes obvious from the study is that quite apart from the health risks of Covid, including the high death rate and the increasing probability of ending up with Long Covid and all the other complications to hearts, brains, livers etc – the bean counters have got the basic calculations wrong.
This graph summarises the scenarios and the relative total costs.

The results of the study are:
1. “Compared to a reference of no admission screening testing of patients and staff surgical masks, all scenarios were cost saving with health gains over a 12-month period”.
2. “the testing or N95 costs were small in comparison to the cost of additional patient bed days due to hospital-acquired infections.”
3. “Staff N95s were cost saving with health gains compared to surgical masks regardless of admission screening …”
4. “PCR admission screening and N95 usage shows the most QALYs gained” – QALYs = total-quality-adjusted life years.
The researchers conclude that while the use of N95 masks and tight admission testing procedures deliver the best health and cost outcomes:
One of the reasons that staff N95 masks and patient admission screening testing have been removed … is the high upfront costs in a context where emergency pandemic funding was removed.
They also argue that with no restrictions in place within the community, more people are checking into hospital for whatever reason who are infected with Covid.
With the lax protocols in place once they are admitted – no special wards etc – they quickly spread the infections to fellow patients and medical staff (who are not using N95 masks), who, in turn, spread the disease more widely both throughout the acute care facility but also back into the community.
Their overall conclusion is that:
… N95 mask use and admission screening testing of patients can save lives and reduce costs related to COVID-19 through reduced patient bed days and staff replacement needs. The more they can practically be implemented the greater the impact is likely to be. Infection prevention and control measures to reduce COVID-19 transmission in acute care settings should continue to be applied.
A definitive conclusion.
The message is clear: trying to ‘save’ outlays by compromising the quality and scope of public infrastructure and services ends up ‘costing’ more over time.
The bean counters celebrate in the short-run their cleverness in cutting ‘costs’ and are mute when the reality dawns that they are actually mindlessly stupid.
And in this particular context – where unnecessary Covid deaths are rising in the hospitals because they have become enclosed infection breeders – the stupidity is in my view criminal.
This ABC news report (May 6, 2024) – Hundreds of patients died after catching COVID in Victorian hospitals, new data shows – summarises the latest available data, which is becoming increasingly difficult to obtain.
Scrutiny of the policy process on this issue is getting difficult because the governments (federal and state) are deliberately suppressing data or abandoning the collection of it.
The Report notes that:
For months doctors and public health experts have been warning that too many patients are catching COVID in Australian hospitals with sometimes devastating consequences — though timely statistics are difficult to access because health departments do not publish them …
Alarmingly, the proportion of hospitalised COVID patients who caught the virus in public hospitals was much higher last year than in 2022 — up from 13 per cent to 20 per cent, on average — coinciding with a reduction in COVID screening and healthcare worker mask use across the state.
In 2023, for example, 2,322 patients contracted Covid from the hospital and more 9 per cent died.
The Report notes that in some cases, people have been admitted to hospital for routine procedures, then become infected with Covid, which, in turn, triggered neurological illness (Huntington’s Disease in the case cited).
N95 mask wearing among the staff was absent in the case cited.
The current research is pointing to the fact that:
The numbers indicate that there is a big problem here — these infections and deaths are potentially preventable
I cannot imagine why we would tolerate that – it is sort of back to the dark ages of ignorance and indifference.
The ABC Report offers some clues.
1. Senior hospital executives think Covid “is just a cold” – they are political appointments and do the work of the bean counters in government.
2. People claim they are “tired of wearing masks” – so why are they not tired of wearing belts or shoes or anything really.
I wear a mask in every setting where there is a risk of infection.
I have grown used to it and it is now routine.
The benefits of not getting sick vastly outweigh the minor inconvenience of wearing the protection.
The fact that the population doesn’t see that reflects the lack of education provided by the government on this issue.
If the general public was apprised of the latest research and its implications for their long-term health then things might change a bit.
And if there was more collective will or solidarity engendered rather than the promotion of rampant individualism then things might change a bit.
There is a reason the Japanese people are high mask wearers – there is a culture of respect and concern for one’s impact on others, that has disappeared in other nations that have been assaulted by neoliberalism.
One hospital that the ABC Report investigated – the Royal Melbourne – has maintained strict testing and mask wearing protocols as well as providing advanced air ventilations technologies and considers – “any sort of nosociomial infection is a disaster”.
So if you ever need to go to a hospital in Victoria try to get in there!
Conclusion
We have been assaulted with federal and state government campaigns against smoking for years.
Road safety campaigns are always prominent and there are advertisements regularly in the media.
Why then has the government gone silent and passive on Covid?
The pandemic is still killing thousands and crippling more.
Our acute care facilities are no longer safe to enter for care.
The risk of becoming infected with Covid and dying in one of these facilities as a consequence is significant and rising.
The policy neglect is actually ‘costing’ government more over time than the short-term cost reductions that accompanied the relaxation of the protocols.
Why then is there policy neglect?
That is enough for today!
(c) Copyright 2024 William Mitchell. All Rights Reserved.
I agree with much of what you write in the above post, however your conclusions were rather interesting in light of a recent lecture I attended by Guy McPherson. You ask why there is policy neglect in light of the pandemic response, but perhaps this was the policy in the first place.
40 years ago, it was a common medical practice – and considered ethical, not to inform a patient of their impending death – or indeed their family members – if the physician considered such news would cause great distress. The right to know has mostly ceased the lack of disclosure, but it’s quite obvious the mushroom growing principle remains in many areas of society. If NASA discovered a large asteroid with a 100% certainty of impacting Earth in two years time, would this information be released at the time of discovery? Not a chance.
Most of the existential threats to our survival are driven by human activity and whatever measures we seek to employ to reduce the impact of our activities and mitigate biosphere collapse that is presently occurring, will depend on a significant population reduction to at least pre-industrial levels to have any prospect of success. At least that was the prevailing opinion amongst many ecologists and scientists about a decade ago, but new research highlights the additional risks of a population collapse to the environment. The reduction in the aerosol masking effect from industrial emissions would lead to a 4.7C rise in the global temperature within two years – then you have nuclear fallout from unattended power plants.
Neither bode well for our chances. There is “no way out” – no answers to what we have created for ourselves. No amount of money, even in an enlightened world will avert the coming disaster; we’ve left it way too late. So I guess a managed decline in population would not be out of the question for policy makers to adopt – just don’t expect them to inform you.
Best Wishes.
How on Earth Could Civilisation and the Biosphere Collapse in the Next Few Years:
https://kevinhester.live/2024/04/07/how-on-earth-could-civilisation-the-biosphere-collapse-in-the-next-few-years/
Professor Guy McPherson on Exponential Growth
https://youtu.be/2jWh6Xjedw8?si=1gQBe4si8yeNi22o
Three cheers for Bill Mitchell! I mean that most sincerely.
Bill continues to “maintain the rage”: a Gough Whitlam quote which in context means to steadfastly maintain one’s moral outrage and social activism and engagement in the face of the most egregious betrayals of the population’s interests by the greedy, callous ruling classes and their willing accomplices.
Everything Bill has written above is correct. The true cost of failing to stop COVID-19 with effective measures and near eradication is far higher than the cost of those layers of effective protections.
An open letter from leading doctors and scientists has recently been sent to the Qld Premier. It covers this ground too and adds further layers of medical and scientific information and references. It contains the most trenchant criticism possible of the Qld CHO and by implication of those who employ and support him. It is very enlightening and well worth reading in full. I recommend it. I hope it is okay to post the link here.
https://www.qldcho.com/
My wife and I also still wear N95 masks everywhere we go in public. We very seldom go into public indoor areas anyway and largely isolate ourselves from society in general. This is partly for medical reasons. My wife and (grown-up) daughter are immunocompromised and suffer from significant medical conditions. Our masking and isolation are partly a protest too, especially on my part. I refuse to toe the line on all the anti-masking denialism and covid-minimising. I refuse to participate (more than I absolutely have to) in all the optional aspects of socialising and spending in a neoliberal, consumerist society that cares nothing about human welfare and nothing about environmental issues and dangers.
So, three cheers again for Bill Mitchell. Many economists seem to have given up on the fight to re-establish sensible health policy for pandemics, preventative medicine and other health matters. Bill does not give up and is prepared to state and demonstrate the truth a thousand times with extensive data each time, should all that be necessary. And in an age of weaponised disinformation that activism indeed remains crucially necessary.
Prevention of infection is the key to avoiding long COVID.
Recent research indicates that the chances of developing long COVID increase with every infection an individual suffers. After a third infection, the chances of developing long COVID increase by about 40%.
Long COVID can have significant effects on all organs (including the brain), alongside its vascular effects.
Zoonotic jumps will increase with the planet’s surface temperature.
John B.,
Yes indeed, prevention of infection is the key. The way to achieve this was and still is to use multiple layers of protection at both the individual and societal levels. Individuals should get vaccinated and boosted, use N95 masks in all risk settings, maintain distance, isolate when possible and properly quarantine themselves if still unfortunate enough to catch it. Governments, instrumentalities and businesses should provide updated vaccines at reliable and medically advisable intervals (not bean-counter determined intervals). They should also provide for proper circulation and hepa filtration of indoor air in all public and commercial settings. The government should provide full and adequate funding and logistics for the universal and free allocation of adequate testing, tracing, masking, air filtering, vaccinations, isolation and quarantining resources.
As the modelling shows, the costs of these programs will lead to net benefits (both economic and in terms of human welfare) by preventing the rampant deaths, morbidity and economic damage of the “let it rip” policy: including preventing the accruing damage from multiple infections and the ever increasing rates of long covid.
If these policies were applied with initial stringency, the time would come when covid-19 was almost eliminated (except for small, isolated outbreaks). Vaccinations, boosters, border biosecurity and some proper quarantine facilities would remain necessary. Clean indoor air, just like clean drinking water, would become the societal requirement and norm with huge attendant savings on illness and on the economic costs of absenteeism etc. Testing and tracing would be reduced to an essential minimum as there would no longer be much covid-19 to test for and trace. Because of the masking and filtering, flus and other respiratory disease would also dwindle greatly in incidence with further big savings.
Sadly, none of this will happen (yet) because it appears people would rather be constantly infected and very often sick than actually be well. This is the conclusion I am forced to. It seems the political economy of our society places such intolerable and unpleasant pressures on most people that they would rather compulsively consume diversions to escape their everyday grind and then constantly get sick as a result. There is something deeply pathological about this sad cycle and it should give us pause to wonder what our society really does to people. In summary, it no longer provides hope for a better future for most and it provides no agency for people to determine their own future rather than have it corporately dictated to them.
However, logically and empirically unsustainable trends cannot be sustained. It is as simple as that. The increasing infections, morbidities and deaths from letting covid-19 rip will prove unsustainable in the long run. Already, it is clear that our domestic and global supply chain difficulties flow in part from a continuous decimation of the global workforce by ever increasing rates of deaths, illnesses and chronic illnesses. There are also many retirements now as people flee the unsafe workforce and its miserable conditions. At some point, so many people will become disaffected because of this ongoing, insidious disaster and all its knock-on effects that they will demand change.
Iconoclast wrote:
“However, logically and empirically unsustainable trends cannot be sustained…….”
I might have written similar a decade ago, but the perspective changes over time. Take 30 mins or so and watch Guy McPherson’s lecture linked in my post above and see if your’s does too.
All the best.
And it’s not just COVID – mask-wearing reduces the chance of getting any airborne virus (hello influenza).
Look at the cases for 2021 compared to the 5 year average in the National 2021 Influenza Season Summary (page 2):
https://www.health.gov.au/sites/default/files/documents/2022/10/aisr-2021-national-influenza-season-summary.pdf
Mark,
That was my clumsy paraphrase of the ironic and sarcastic “Stein’s Law” which states: “Things that can’t go on forever, don’t.”
Exponential growth on a finite planet cannot, of course, go on forever. Guy McPherson has been warning about this for decades just as the Limits to Growth authors did.
I think Guy McPherson is correct in saying that we are on a trajectory or even already past the point of no return to massively destabilise our climate. This will likely occur in a way that leads either to runaway global warming or else to a more chaotic weather era (more chaotic than the Holocene era) of unknow duration followed perhaps by a new (and also ultimately temporary) climate state.
“The climate system is a coupled non-linear chaotic system, and therefore the long-term prediction of future climate states is not possible. Rather the focus must be upon the prediction of the probability distribution of the system’s future possible states by the generation of ensembles of model solutions.” – IPCC.
What we can’t know yet is the starting point and span of time in which one a transition will take place. Guy McPherson seems certain that we will know indubitably by 2030 that one of the above catastrophic transitions has commenced. I would say, the system is too chaotic for us to know or calculate that. In chaotic systems small changes in initial conditions can make huge changes in final conditions. That makes picking such a clear and near date a little dubious. But I can’t be certain either. Guy McPherson may turn out to be right. I am certainly not an expert in such matters. Concerning trends seem to be accelerating terrifyingly quickly.
But the topic was COVID-19 myopia and I don’t want to go too far off-topic. Of course, the topics are linked, Covid-19 myopia and climate change myopia have at least one major proximal cause in common and that is neoliberal economics. Neoliberal economics puts up its definitions of “sound money” and “fiscal responsibility” as policy goals above real things like having a sound environment and sound climate.
Reading “It is obvious that massive savings to government arise from scrapping any mandates to wear N95 masks and to screen for Covid on admission.” makes me think that heterodox economists of the MMT kind can be their own worst enemy. In saying such things as “government savings” when the currency issuer saves nothing because it has the power to issue the currency anytime at its own choosing seems to play by the rules of the orthodoxy. Financial savings mean nothing, zilch, zero to any government that has its own currency issuing monopoly power whereas choosing where to spend is/should be/must be the real concern of such governments.
Words matter. And in that vein I would like to propose that the following be observed, if not absolutely clear from the context of their use:
Investment should always be qualified as being for:
(i) productive purposes; or
(ii) asset purchases
Debt should always be qualified in use as:
(i) public; or
(ii) private
Inflation should always be qualified as:
(i) demand-side; or
(ii) supply-side
and
(i) persistent; or
(ii) transitory (not necessarily very short term)
Fred:
Asset purchases for pure capital gain are not a form of investment. They are a form of savings. All investment spending in the strict sense of the word is for productive purposes.
In my opinion, a debt occurs when, in order to extinguish a liability, one must give up something that is real and has use value. Currency-issuing central governments issue liabilities not debts. They have 100% seigniorage and give up nothing to create the base money they spend to obtain real stuff (real resources, labour power, and finished goods and services). All liabilities of currency users, whom have 0% seigniorage, are debts. The liabilities of currency issuers are not.
Thanks Phil. I can agree with what you say at an academic economist level of understanding of investment. However, that is not how “investment” is discussed out in the real world of the currency user taxpayer of you and me. The destruction of western manufacture (neoliberal globalisation) and the rise of Ponzi finance rentier capitalism where the highly visible FIRE sector makes clear that our economy is comprised of production on one side and asset price inflation/deflation on the other. Notwithstanding that “All investment spending in the strict sense of the word is for productive purposes.” I am contending that we need to talk of such things, perhaps in different ways within and without professions in dependence upon the audience.
I see that economics, like all professions, has its own way of talking amongst itself that gets shorthanded while being definitionally lost in translation when discussed outside that profession. I practised patent law where clients came with a belief that a valid patent grants an unfettered monopoly right to manufacture what is patented. While correct at the level of being able to stop infringers of a valid patent, that right is qualified by the logic that such is only available for no risk exploitation where exploitation of what is patented is free from infringment of any other party’s earlier in force prior valid patent right that would be infringed if that later patent were to be commercially exploited.
I can also acknowledge and appreciate your academic perspective on debt. That government currency issuers incur debt, but only on an accounting/record keeping basis and not on a “spend to obtain real stuff (real resources, labour power, and finished goods and services)” on the condition that “one must give up something that is real and has use value.”. While seeing what you’re getting at, that is not how the matter is discussed by the corporate propagandising media, politicians or orthodox economists and as parroted back by the indoctrinated masses on the non-government side of the economy. If heterodox economists are to get their message across to the many I think that they need to be using the language and understandings of their audience and not those used just within their professional lexicon. What do you think?